OR Microscope

Steps of cataract surgery and potential complications
Major Steps of Surgery
1. Surgical Wounds
- 3-wound approach
- BSS/OVD to create space + protect intraocular structures
(0:24-1:10)
2. Capsulorhexis
- Mark cornea with rhexis ring → capsulotomy → capsulorhexis
(1:13-2:00)
3. Hydrodissection
- BSS canula just deep to anterior capsule → fluid wave around cataract
(2:13-2:30)
4. Phacoemulsification
- Divide & conquer technique shown here
(3:20-6:16)
5. Irrigation + Aspiration
- Bimanual technique shown here
(6:29-8:29)
6. IOL Insertion
- Enhanced monofocal placed within capsular bag
(8:58-9:32)
Key Concepts & Definitions
BSS | Balanced Salt Solution
- Sterile, isotonic saline used intraocularly, on anterior corneal surface, and in wound closure.
OVD | Ophthalmic Viscosurgical Device
- Dispersive, cohesive, or mixed material injected into the eye to protect intraocular structures and occupy space during surgery.
OR Microscope
Dilation | Pupil should be dilated to >6mm
Purpose
Allows adequate size field for
- Retroillumination, capsulorhexis, and IOL placement.
Standard Pharmacologics
- Phenylephrine or Tropicamide drops pre-operatively
- Can give dilute epinephrine intra-operatively to help with poor dilation.
History
- Pseudoexfoliation syndrome
- Pigmentary dispersion syndrome
- Prior intraocular surgery
- Anterior chamber inflammation
- Drugs causing Floppy Iris
(Tamsulosin, Doxazosin, Terazosin, Ropinirole, Saw palmetto)
Exam findings
- TIDs
- Posterior synechiae
- Iris coloboma
- Irregular iris shape
- Intraoperative Floppy Iris Syndrome (IFIS)
- Anterior capsule damage
- Inadequate field of view for surgery
Complication Prevention
1. Iris hooks or Malyugin ring
Example |
Indications |
Benefits |
|
|---|---|---|---|
Malyugin Ring |
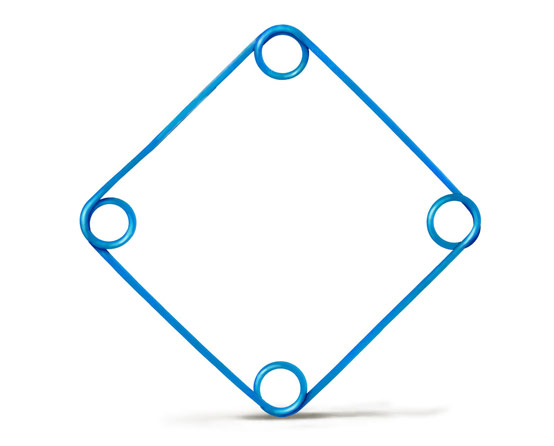 |
Pupil dilates to < 6mm |
Equal tension throughout iris circumference Malyugin ring comes in 6.25 mm or 7 mm |
Iris Hooks |
 |
- Intraoperative Floppy Iris Syndrome eg, Iris colobomas |
- Allows for customized placement *Subincisional iris hook is also a good way to prevent iris prolapse |
*These should NOT be used until concern for posterior synechiae is eliminated/resolved.
2. Synechiaelysis
Retroillumination | Red Reflex
Purpose
Intraocular structure visibility
- Achieve with microscope lighting
Allows visual differentiation of lens capsule versus cortex.
Red reflex must be present
- Presence of P1 of purkinje light reflex does not equate to adequate retroillumination.
History & Exam
- Endothelial loss
- PSC or Intumescent cataract
- Keratopathies
- Stromal edema
- Posterior polar cataract
- Retinal atrophy
- Significant astroid hyalosis*
*Theoretically this could make visualization more difficult, but highly unlikely in practice.
Methods to improve surgical view
Use a capsular dye
(Trypan blue, Iridocyanine green)
Adjust microscope setting
for more coaxial lighting and less oblique lighting
Scrape the epithelium off
if corneal scarring/edema preventing view
Use an external light pipe
with the microscope light turned off
Chandelier assisted retroillumination
Surgical Wounds | Primary + Paracentesis
Purpose
Lens removal and implant placement
- Provides control and manipulation of intraocular structures.
Paracentesis
1-2 incisions
In addition to primary wound
Number
- Depends on OVD & cortex removal method
Location
- Limbal vessels, usually 12:00 & 6:00 on cornea
- Depends on patient anatomy (eg, presence of tube shunt) and ergonomic efficiency.
Function
- Provides delivery route for intra-cameral epinephrine, lidocaine, OVD, and BSS.
- Entrance point for I&A handpieces.
Instrument
- Steel paracentesis blade (1.0-1.2 mm)
- Reusable diamond knife
Location
- At limbal vessels
limbal vessels promote wound healing during post-op.
Primary Wound
Instruments

Keratome
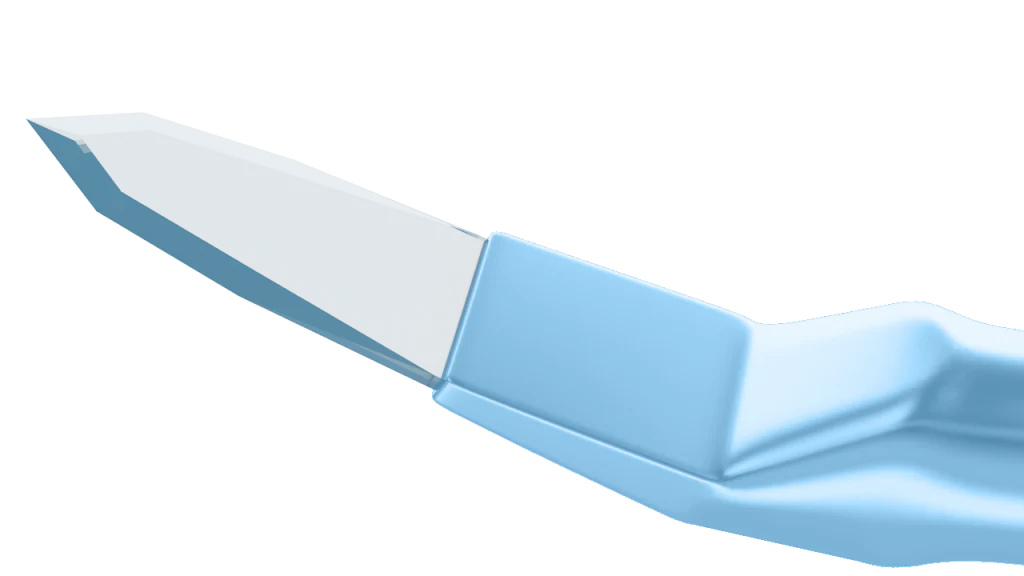
Diamond blade
Location
- Temporal cornea, usually just superior or inferior to 3:00 or 9:00 due to ergonomic dominant hand positioning
- Closer to 8:00 for right eye, 2:00 for left eye.
Shape
- Square shaped wound (from microscope POV)
Incision Types
1. Clear Corneal Incision (CCI)
- Biplanar
- Triplanar (most commonly used)
2. Scleral Tunnel
History
- Neurotrophic keratopathy
- Corneal ectatic disorders
- Corneal transplant
- DES
- Corneal dystrophies
- Ocular sequelae of systemic disorders
- Limbal stem cell deficiency
- Cognitive or intellectual disorders (preventing post-op compliance of not rubbing eye)
Exam Findings
- Corneal epithelialization
- CCT > or < 520-560µm
- Stromal edema
- Confluent PEEs
- Corneal neovascularization
- Surgically Induced Astigmatism
- Postop wound dehiscence
- Epithelial downgrowth
- Iris prolapse
- Anterior capsule nicking
- Descemet's tear
Complication Prevention
Optimize wound parameters
IOP + OVD | Protecting anterior chamber structures
Purpose
Maintain spaces and protects endothelium
- Open wound creates exit for aqueous fluid, allows fluctuations.
Allows fluctuations in anterior chamber depth.
History
- Intraocular surgery
- Intraocular inflammation
Exam Findings + Preop Measurements
- Shallow ACD (<3.2mm)
- Narrow angles
- Poor dilation
- Irregular or damaged pupil
Intra-operative
- Large surgical wound
- Insufficient pupillary dilation or tension
- Extended period of high phaco settings
- Phacoemulsification above the iris plane
- Posterior chamber pressure >> anterior chamber pressure
- Capsule compromise
- Corneal endothelial loss
- Iris prolapse
- Corneal edema
- Rapid changes in zonular tension resulting in damage
Complication Prevention
1. Maintain AC and intracapsular space
2. Maintain pupillary dilation
3. Adequate endothelial protection
Capsulorhexis | Removal of anterior capsule
Purpose
Allows access to inner lens structures.
1. Mark anterior corneal surface with rhexis marker
Instrument options
- Koch rhexis marker
- Wallace capsulorhexis gauge
1. Use distance from mark to iris (when eye is centered under lighting) instead of the mark itself to guide rhexis.
2. Larger rhexis size for dense/brunescent cataracts (~≥5.5mm).
- Creates more space to work with the inevitably stiffer lens fragments associated with brunescent/dense cataracts.
- Eye moves during rhexis/intra-ocular manipulation. This changes external corneal surface relationship/angle to anterior capsule from surgeons POV. Corneal mark will not remain over the exact location the rhexis should be.
2. OVD in AC
Choice of dispersive vs cohesive depending on concern for run-out.
3. Capsulotomy
Instrument
- Cystotome
Wound starts from anterior capsule's center and extends radially ~2-3mm.
- Puncture central capsule, create flap via push or pull techniques

4. Capsulorhexis
Instrument
Capsulorhexis forceps
Pull anterior capsule tissue closest to the free tissue's base & pull in cuvilinear direction.
- Creates symmetric, circumferential wound of ~4mm diameter around center of capsule.
Maintains equal tension of surrounding zonules and ensures capsule will in the same position.
History
- Intraocular inflammation
- Zonulopathy
- Pars plana vitrectomy
- Pseudoexfoliation Syndrome
- Pigmentary Dispersion Syndrome
- Ocular trauma
- Hypermature cataract (eg, morgagnian)
Exam Findings
- Mature or intumescent cataract
- Posterior polar cataract
- Phacodonesis
- Posterior synechiae
- Incongruency in expected anterior chamber depth and axial length
- Radial tear during rhexis
Occurs as a result of excess to posterior pressure exerted on lens during rhexis
- Bag break (eg, Argentinian Flag Sign)
- Asymmetric rhexis
- Rhexis > 6mm
- Rhexis < 4mm
- Risk factor for phimosis
Complication Prevention
Retroillumination/Red reflex
- Improves visualization and depth differentiation of intra-ocular structures.
Trypan Blue (eg, VisionBlue) or Iridocyanine green
- Improves visualization and differentiation of lens capsule during capsulorhexis when retroillumination is not sufficient.
Hydrodissection | Separate cataract from capsule
Purpose
Mobilize cataract
- Reduces amount of energy required to remove nucleus.
Reduces risk of phaco energy-induced complications.
Complication Prevention
Capsular retention hooks for capsular support in zonulopathy
See above (Capsulorhexis) for same complication risk factors.
Hydrodissection complications involve capsule damage or break.
Capsular Retention Hooks
Usually place prior to hydrodissection,
(after capsulorhexis)
- Relieves uneven capsular bag tension
- Stabilizes capsule with minimal zonular stress
- Provides anterior and posterior capsule support
- Prevents capsular torquing
MST capsule retractor - Chang modification (beye.com)
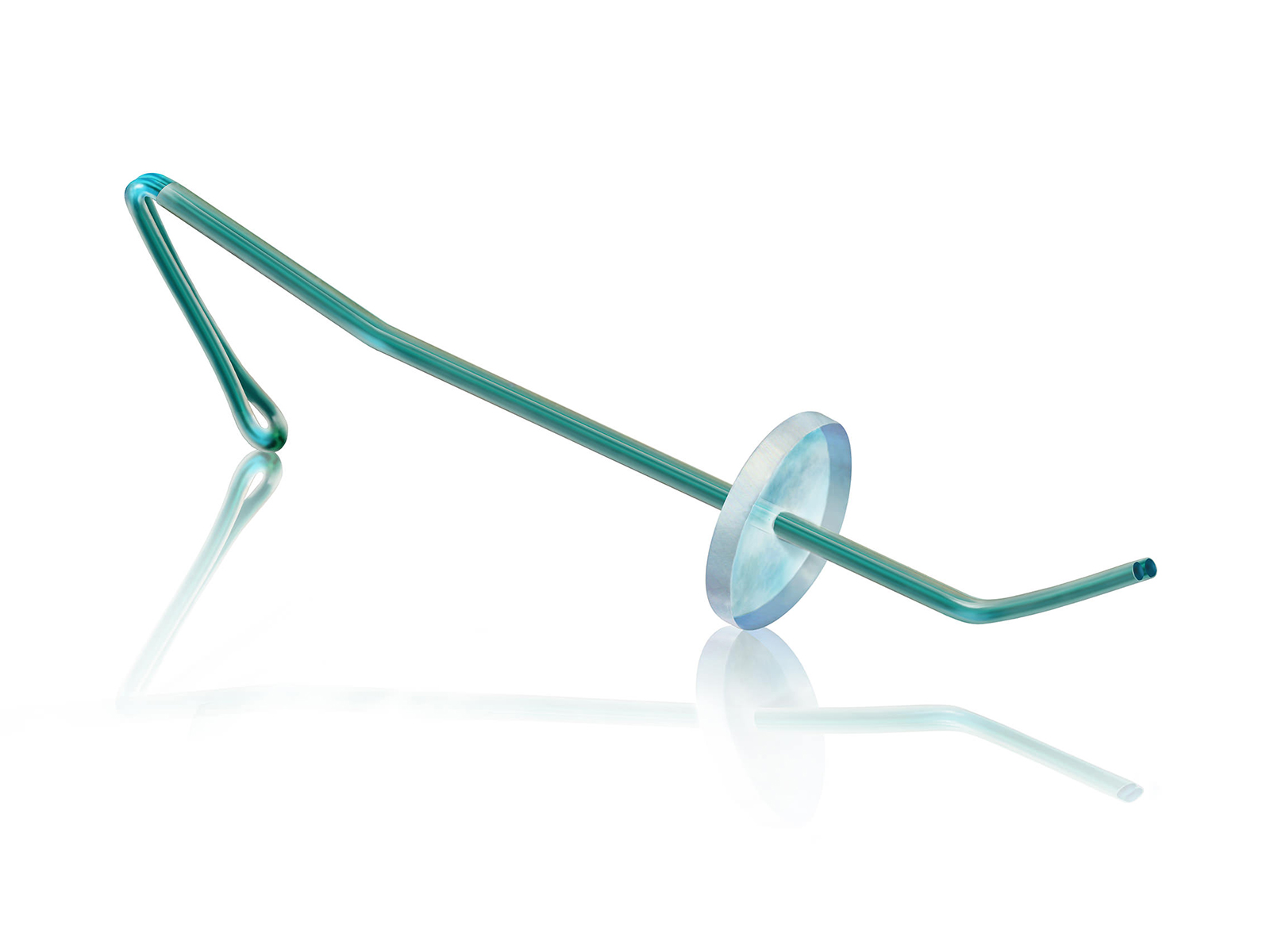
Capsular Tension Ring or Segment
Ideally placed during the latest possible step
(after I&A / polishing).
- Relieves uneven zonular tension
- Provides additional long-term zonular support


Capsular Tension Ring (imt-usa.com)
Morcher Ahmed Segment (FCI-ophthalmics.com)
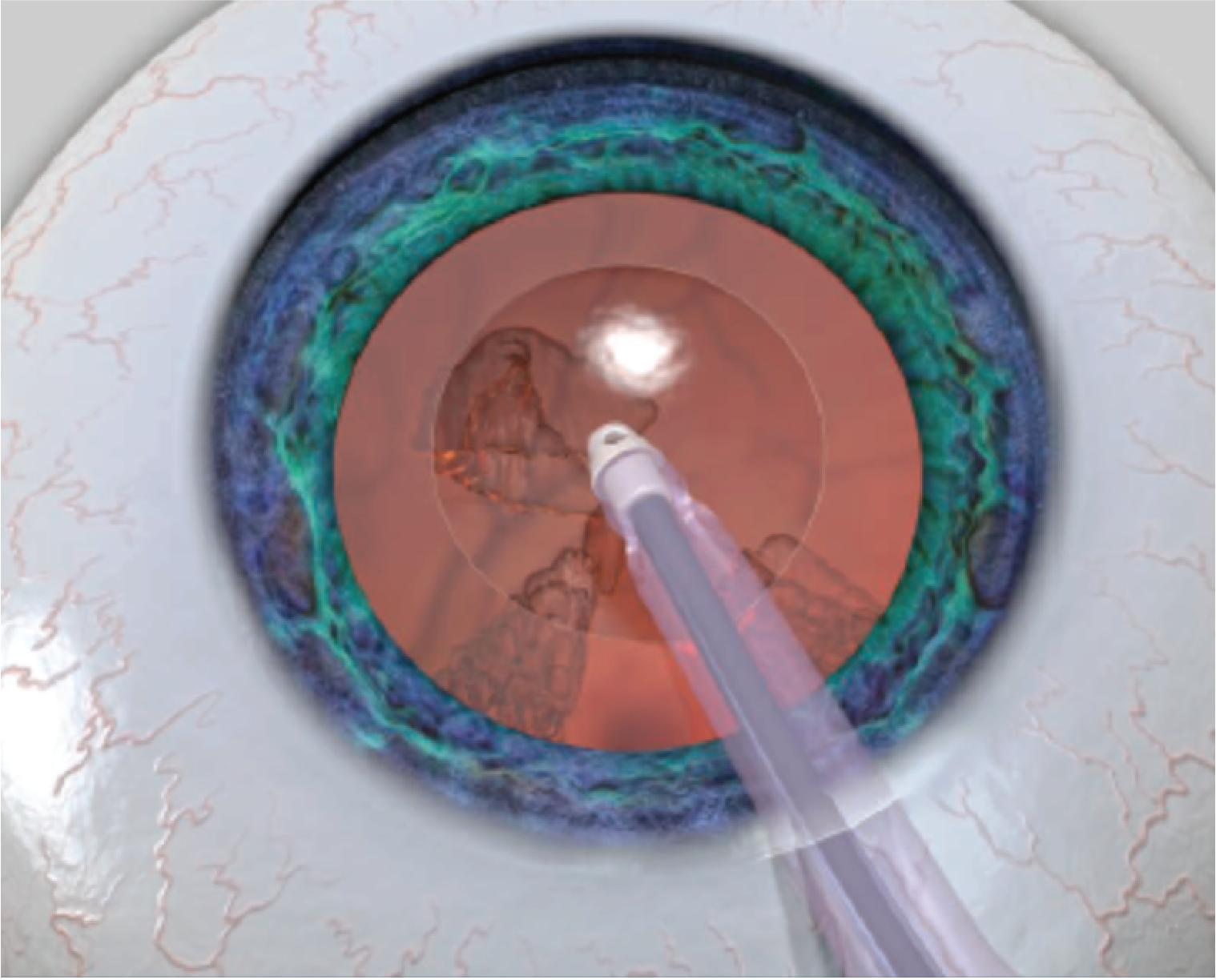
Phacoemulsification | Nuclear dissassembly
Purpose
Nucleus removal

Pedal Settings & Appropriate Use
Position 1
Irrigation only
Maintains chamber volume
- Continuous irrigation option
- Height of infusion bottle determines irrigation infusion rate
Use During
Cataract emulsification and Irrigation + Aspiration
Position 2
Irrigation + Aspiration
Linear control of flow and vacuum
≥1/3rd down
Mechanism depends on brand
1. Peristaltic (Centurion): vacuum builds when phaco tip is occluded
2. Venturi (Stellaris): vacuum created instantly
Use During
Cataract emulsification and Irrigation + Aspiration
Position 3
Irrigation + Aspiration + Phaco
Full irrigation + aspiration & control of phaco energy
≥2/3rds down
Use During
Cataract emulsification only
Modes
1. Continuous
2. Pulse
- Alternating phaco-on phaco-off time
3. Burst
- Time interval between bursts is dependent on foot pedal depression
- More depressed = shorter phaco off-time & more phaco energy
Settings
Sculpt |
Chop |
Quadrant Removal |
Cortex or Epinucleus |
Viscoelastic Removal |
|---|---|---|---|---|
- Low vacuum - Low flow |
- High vacuum - High flow |
- High vacuum - High flow |
- High vacuum - Moderate flow |
- High vacuum - High flow |
History
- PPV history
- Endothelial damage
- Drugs associated with Floppy Iris
Exam Findings
- Posterior polar cataract
- Zonulopathy
- Endothelial damage or wound burn
From high phaco settings, phaco for too long, or using phaco too close to cornea
- Zonular damage, dialysis, or capsule compromise
From vacuuming capsule
- Iris prolapse from excess intraocular irrigation force
From excess intraocular irrigation force &/or inadequate mydriatic pharmacologics
Complication Prevention
Phaco in iris plane
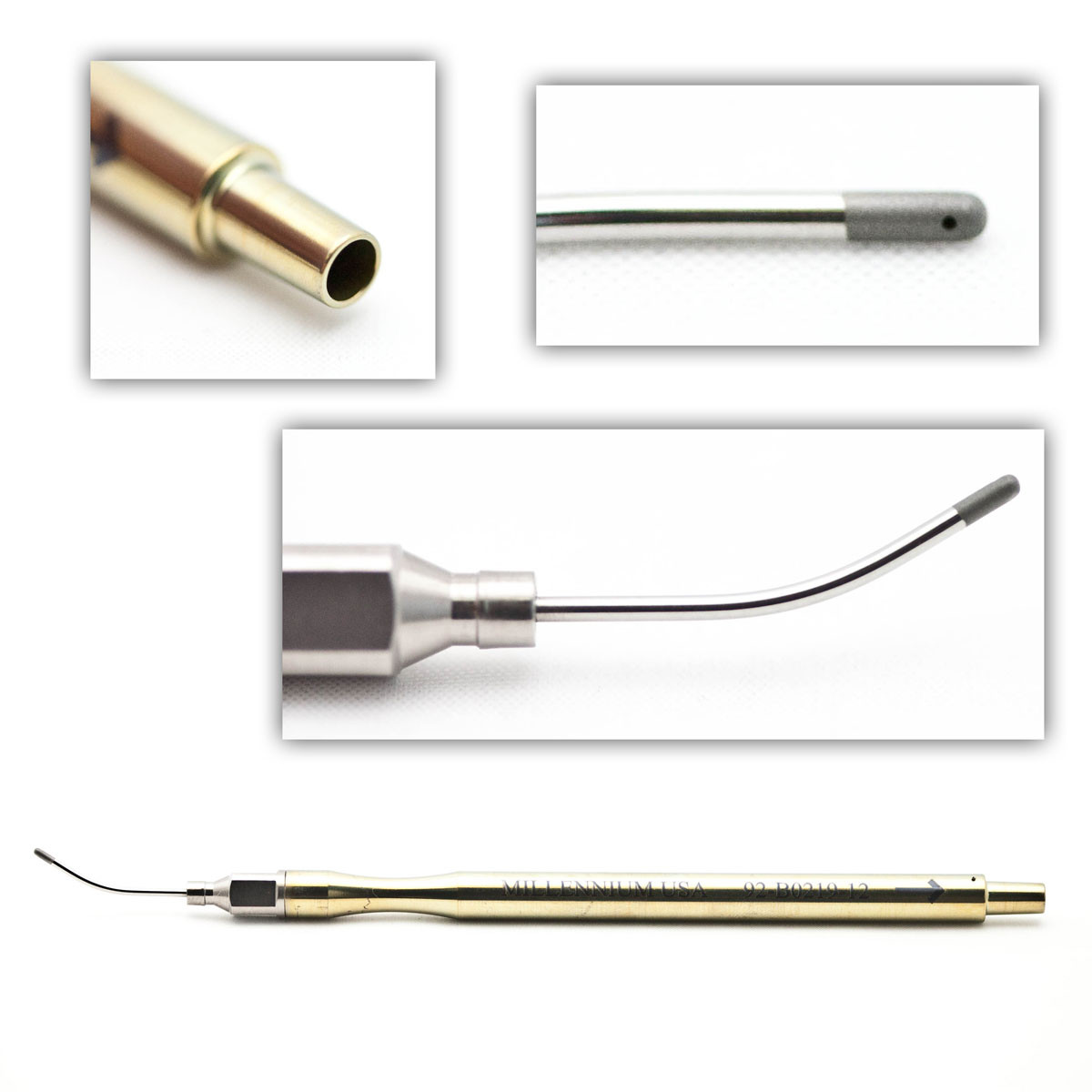
Miloop
Koch Spatula
Wound Burn and Endothelial Damage Prevention
Phaco should not be used while exiting wound, near wound, or near corneal endothelium.
- Point phaco tip away from endothelium
- Ensure phaco sleeve is protecting the cornea/wound
Prevent Added Zonular Damage
Maintain neutral position in paracentesis with second instrument to prevent unstable fluidics.
Keep eye in neutral position, avoid chasing globe.
Reduce Energy Required to Remove Lens
miLOOP
- Used for very dense cataracts.
- Manually separates nucleus to allow removal without excess energy.
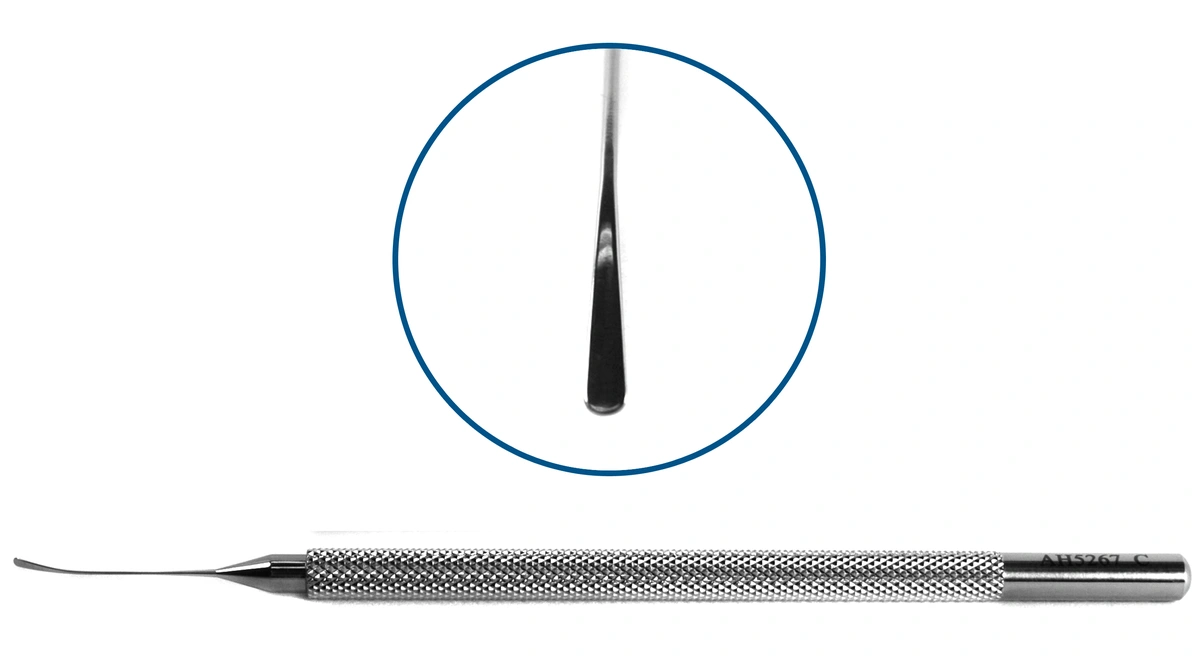
Protect Posterior Capsule
Position Koch Spatula under last nucleus fragment.
- Reduces energy that posterior capsule absorbs from phacoemulsification.
Ziess miLOOP (mivision.com.au)
Koch Phacoemulsification Spatula (accutome.com)

Irrigation + Aspiration | Cortex removal
Techniques
Bimanual vs Coaxial
Instruments/Techniques
Bimanual
•More controlled, slower technique for removing cortex.
•Better for eyes with zonulopathy risk factors.
•Sub-incisional areas of capsule are more easily accessible.
Coaxial
•Faster, more efficient.
•Higher flow and vacuum settings.
•Requires stable zonules.
Tips for Cortex Removal
Primary technique:
1. Occlude tip with cortex under anterior capsule edge
2. Slowly pull towards center to peel cortex out
Alternative Technique:
Side to side sweeping
- Allows removal of more material
- Ensures tip is occluded
(instead of 'fishing' for specific points within the capsule)
Complications
1. Pigment cells loss.
Iris pressing against cornea can cause this.
Prevention
- Combined OVD in sulcus:
Added benefit of preventing corneal edema/damage while still creating space at the angle
2. Retained lens material
Prevention
Ensure entire cortex removal via side-to-side sweeping technique.
Option to Polish Anterior & Posterior Capsule
Instrument Options
1. Bimanual & Aspirate
2. Singer Sweep
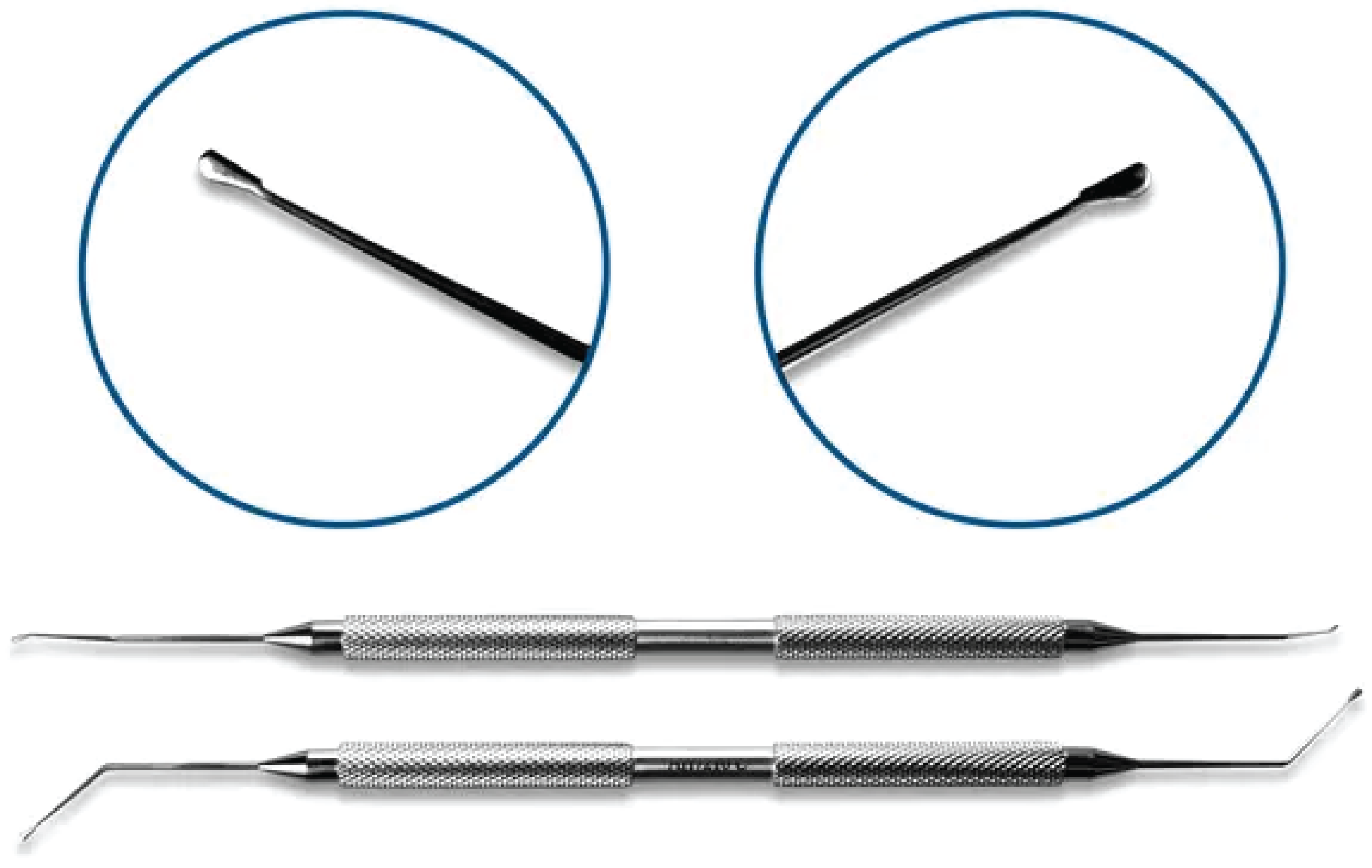
Accutome.com
Anterior Capsule Polishing
Irrigate to remove residuals on posterior capsule
Pros
- Prevents phimosis
Irregular capsule contraction resulting from lens epithelial cells contacting implant.
- Long term improvement in zonule strength
Contraction isnt pulling on zonules
Cons
- Can result in negative dysphotopsias
IOL Insertion
Complication Prevention
Zonular support

