Haptic Configuration
3 Piece
Pros
- The only IOL style that should be placed with haptics in the ciliary sulcus.
Haptic Design
- Rigid and short
- Loop
Optic Material
- Acrylic or Silicone
Placement
- Capsular bag
- Ciliary sulcus
With or without optic capture.
- Secondary IOL fixation
Several techniques for this.
Visual References
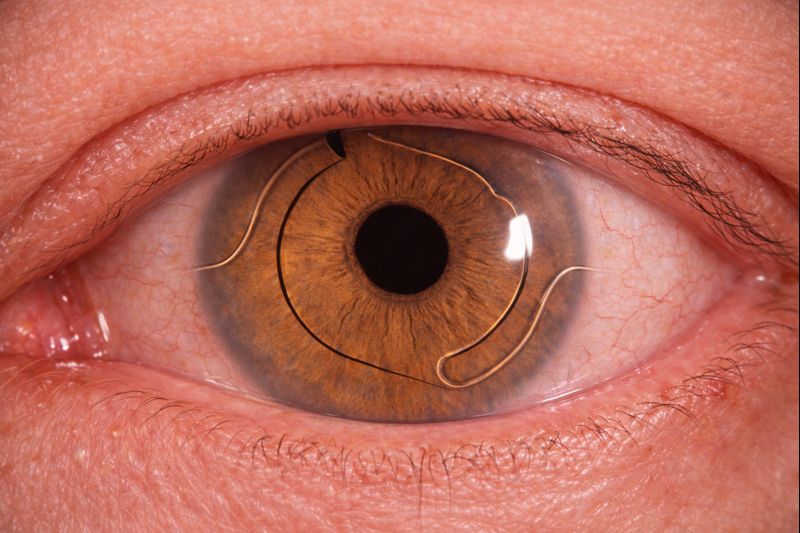
Haptic Characteristics

3 piece vs 1 piece IOLs
The IOL on the left is a 3 piece IOL.
All 3-piece IOLs have loop haptics.
The IOL on the right is a 1 piece IOL.
1-piece IOLs can have either loop or plate haptics.

1-piece IOLs with plate haptics.
IOL Placement
Anterior Chamber Placement
These IOLs are designed specifically for AC placement and cannot be placed in the posterior chamber.
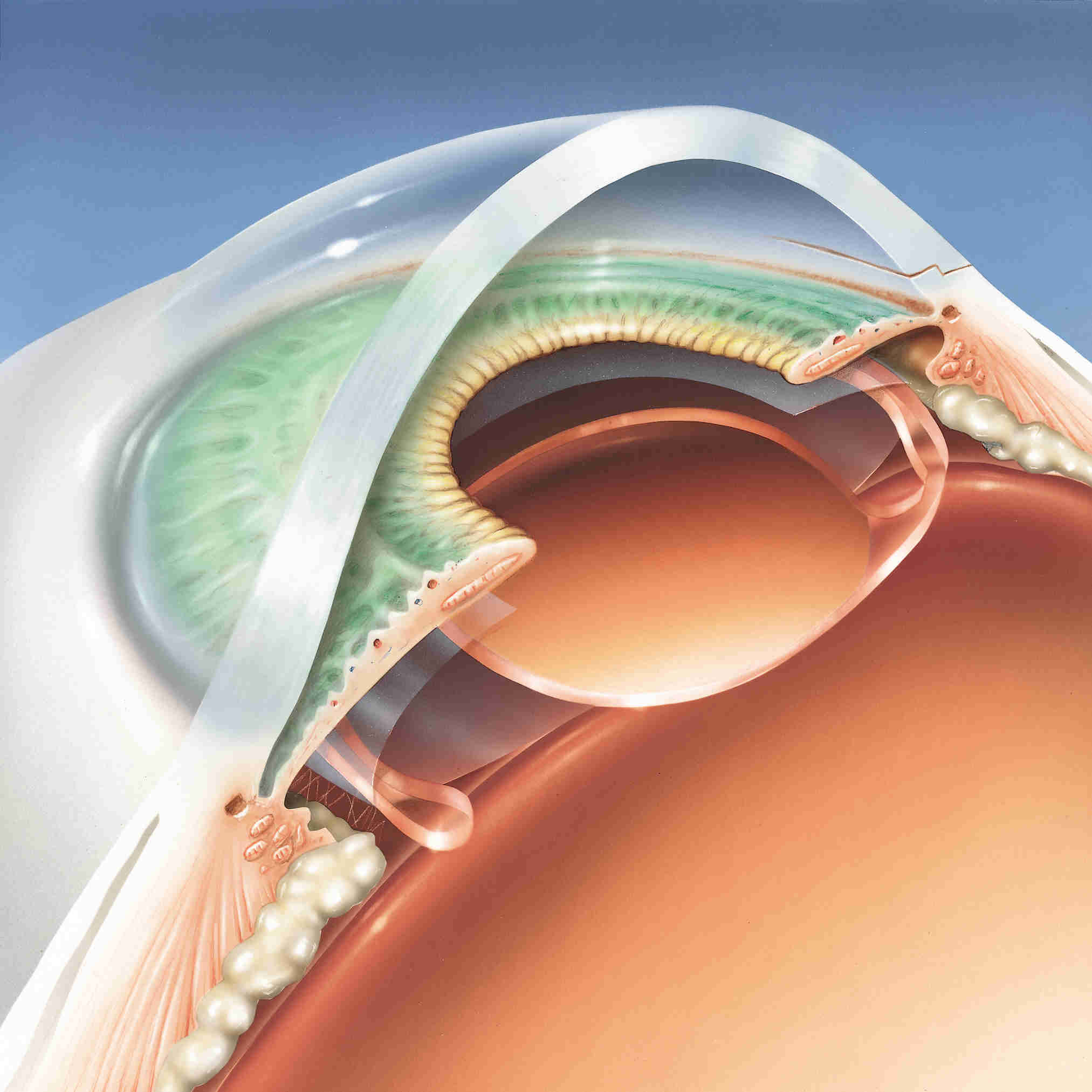
Capsular Bag Placement
In the posterior chamber.

Ciliary Sulcus Placement
In the posterior chamber.
1 Piece
Pros
- Usually square edge design.
Limits PCO formation.
- Less trauma to capsule.
- More uniform contact/tension within capsular bag.
Reduces amount of capsule wrinkling.
Haptic Design
- Flexible and long
- Loop
- Plate
Optic Material
- Acrylic
- Silicone
- PMMA
*PMMA IOLs do not fold and require larger incisions.
Placement
- Capsular bag
- Anterior chamber
Some PMMAs IOLs are specifically designed for anterior chamber placement.
Should NOT be placed in ciliary sulcus
- Risk of Uveitis-Glaucoma-Hyphema syndrome (UGH).
- Unstable placement; lens can shift over time.
Material & Properties
Influence A-Constant
Silicone
Foldable
Pros |
Lower incidence of dysphotopsias
- From lower incidence of refraction.
Cons |
Thicker Optic
- Slippery to grasp.
IOL can become opacified
- Slippery to grasp.
- When in contact with silicone oil or gas.
Caution for eyes with retinal detachment risk factors.
Acrylic
Foldable
Hydrophobic
More common
Cons |
Higher rates of dysphotopsias
Hydrophilic
Pros |
Better visual quality
Cons |
More likely to develop calcifications
Shape
Optic Profiles
Influence A-Constant
Biconvex
- Majority of IOLs
Most IOL calculations assume biconvex lens use.
- Lens power is split between front and back of lens.
Optic Profiles
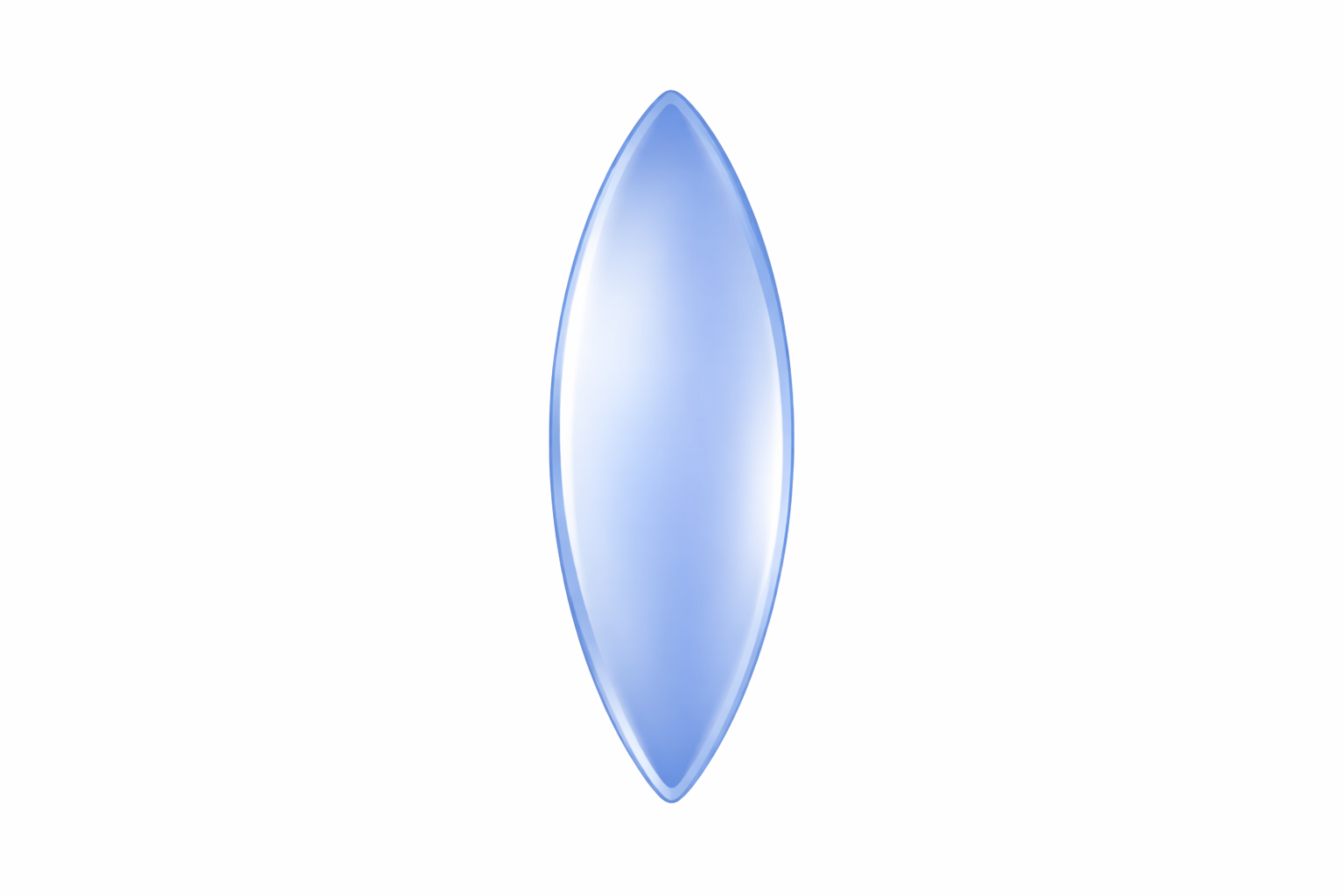
Biconvex
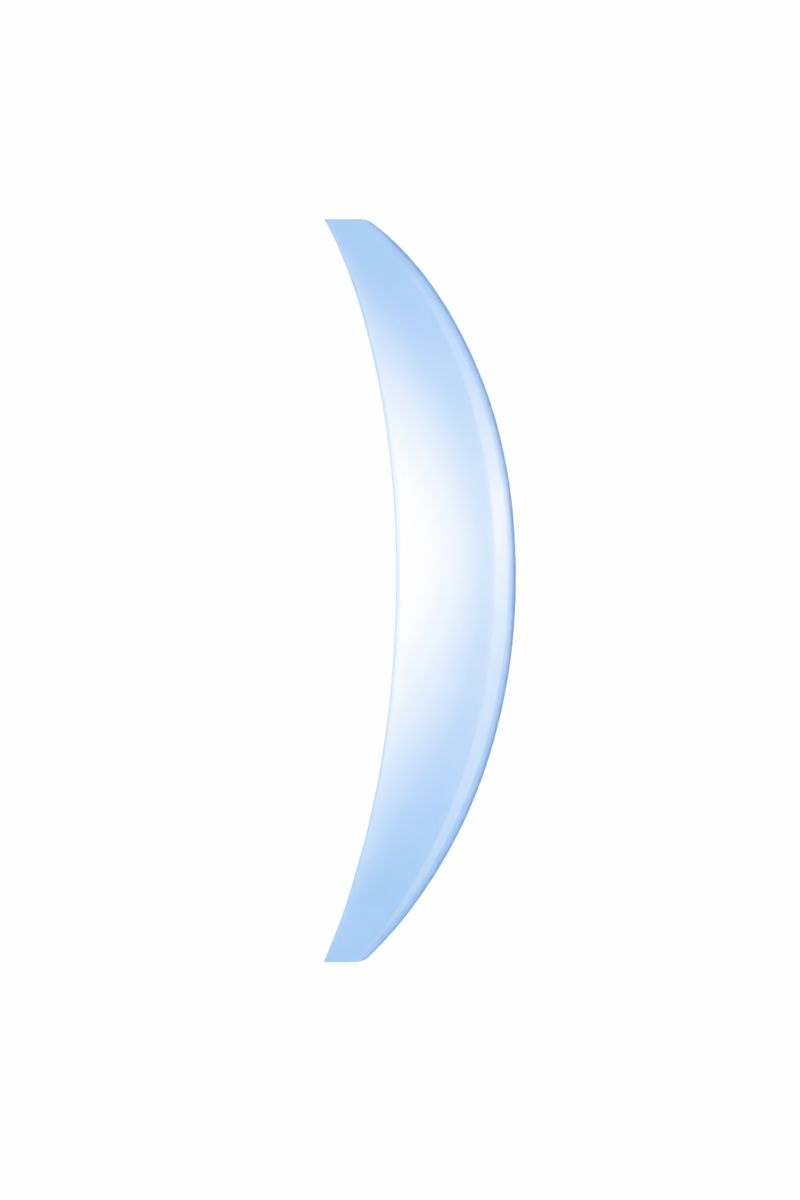
Meniscus
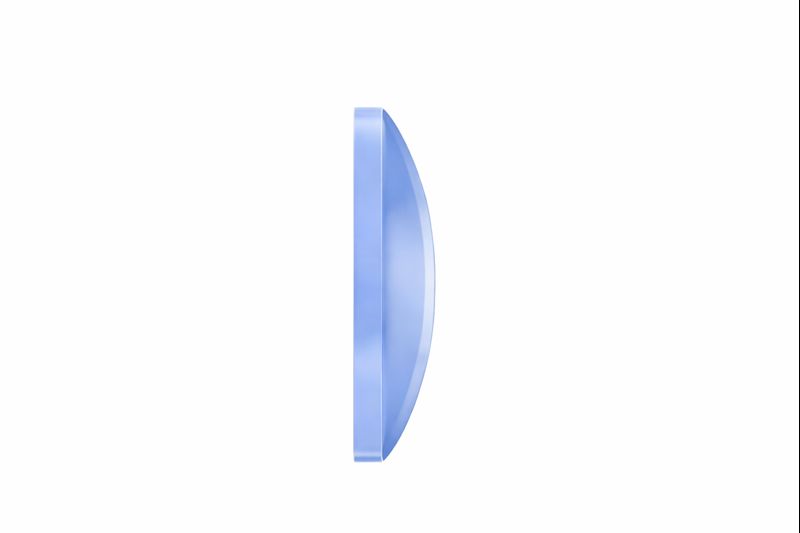
Plano-convex
Meniscus
- Meniscus shape is required for low- and negative- IOL power.
Highly myopic
Long axial length
High K values
- IOLs with these diopter ranges
- MA60MA
- AR40e, AR40M, AR40E
- Best fit formulas
- Barrett II formula
- Ladas 2.0 Artificial Intelligence
Plano-convex
- Primarily used in status-post PPV patients who have silicone oil in the vitreous cavity.
Flat posterior surface of IOL decreases likelihood of refractive surprise.
- Lens power is only from anterior surface of lens.
- Non-foldable/Non-injectable.
Require large scleral wound.
Sphericity
Influence A-Constant
Considerations
Corneal spherical aberration profile: +0.27.
Myopic LASIK/PRK: (-) spherical aberration IOL preferred.
- Cornea is flattened.
Increases (+) spherical aberration of cornea.
Hyperopic LASIK/PRK: Neutral spherical aberration IOL or (+) spherical aberration IOL preferred.
- Cornea is steepened.
Causes (-) spherical aberration of cornea.
Aspheric Lens
Aspheric anterior surface of lens.
Most have negative spherical aberration power.*
- Helps negate cornea's (+) aberration.
- Increases depth perception
(Technis: -0.27, Alcon: -0.21)
IOLs with Neutral spherical aberration profile
- Bausch & Lomb enVista Monofocal IOL (MX60E)
*Less likely to contribute to visual disturbances.
Spheric Lens
Spheric anterior surface of lens.
Most contribute to (+) aberration.*
IOLs with neutral spherical aberration profiles.
- Alcon (SA60AT)
*More likely to cause visual disturbances.
Optic Edge
Sharp Edge
Lens edge is squared/truncated
- Less likely to cause PCOs.
Lens Edge Characteristics
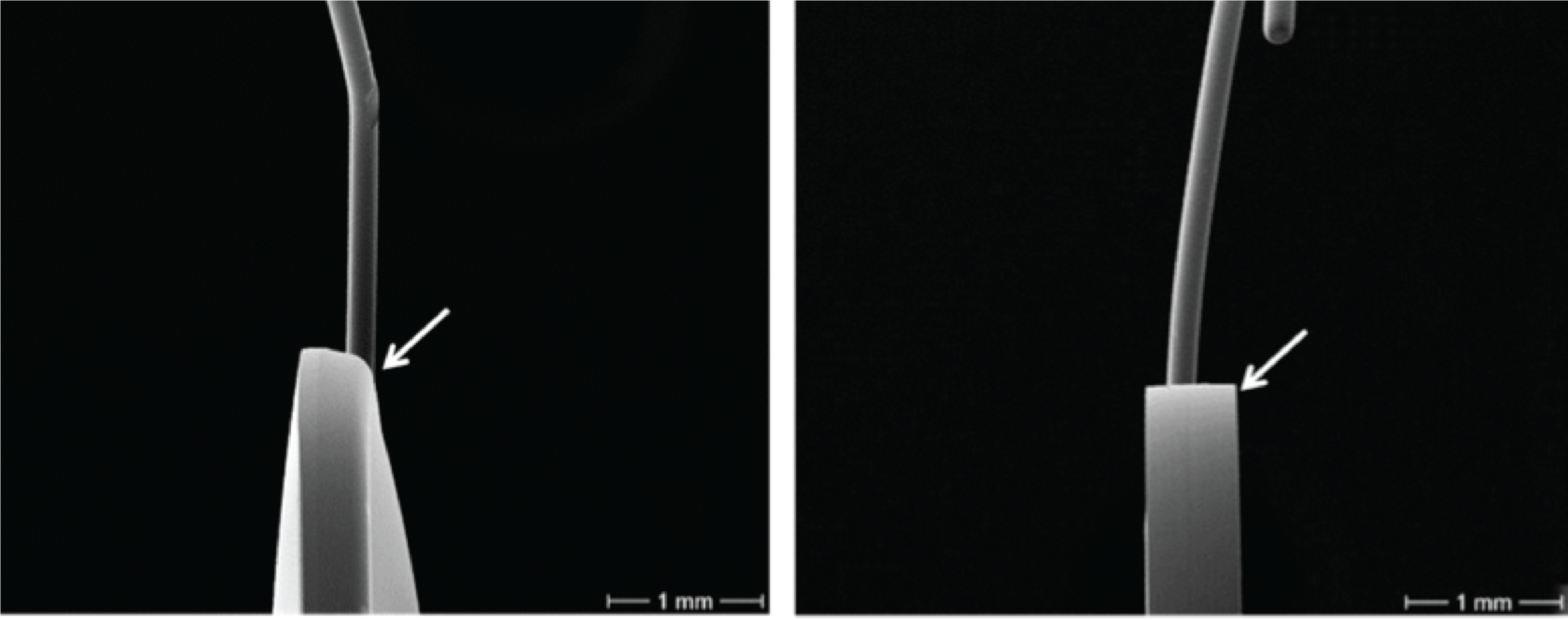
Rounded Edge (left) Sharp Edge (right)
Nguyen et al 2017 Webvision
Rounded Edge
Lens edge is rounded
- More likely to cause PCO.
Haptic Edge
Square Edge
Best for intra-capsular IOL placement.
Rounded Edge
Best for ciliary sulcus placement.
Rounded haptic edges reduce the risk of iris chafing.
Iris chafing results in iris pigment loss and peripheral TIDs.
Comorbidities
Compromised Capsule or Zonule Integrity
3-Piece IOL
- Offers more placement options in case the capsular bag has a posterior tear or zonular compromise.
Toric or Multifocal (MF) IOL
- May not be suitable if centration cannot be guaranteed.
Inflammatory Pathologies
Acrylic Material
- Associated with less post-op inflammation.
Silicone Material
- Avoid due to calcification risk.
Retinal Pathologies
Relative contraindication for MF lenses.
- Affects vision quality + contrast sensitivity in patients with retinal pathologies.
*MF IOLs provide less light transmittence to posterior chamber.
Refractive History
Refractive surgery using older methods | RK, Hexagonal Keratotomy
Problems to Consider
- Irregular astigmatism
- Fluctuations in refractive error throughout the day.
Selecting an IOL for RK patients
Avoid MF IOLS in RK patients
- High risk of dysphotopsias
- RK eyes already have high (+) spherical aberration
Ideal IOL options for RK patients
- Monofocal IOL aimed at slight myopia
- LALs
- IC-8 Aphtera IOL in non-dominant eye
IC-8 Aphtera acts as a pinhole and filters out peripheral light rays, ideal for corneas with peripheral scars (eg, previous RK).
Appropriate IOL Formulas
Use ASCRS IOL calculator for post-refractive patients
Underestimate IOL power (target slight myopia)
- Barrett true K shows best concordance in this calculator.
Patient Goals
- What are the primary activities of daily living for your patient?
- Are they working on a computer or spending most of their time driving?
- Are they a photographer or painter?
- Has your patient ever worn glasses?
- Do they want to continue wearing glasses?
- What level of spectacle independence would they like to have?
- Do they mind wearing reading glasses?
- If they are a myope, how important is keeping their ability to see near without glasses to them?
- Have they previously done monovision through CL or refractive surgery?
- Was this successful?
- Do they have the CL Rx for us to confirm?
- How bothered are they or would they be by glare/starburst at night?
- Do they drive at night frequently?
- What is your patients' financial understanding?