Indications
Clinically Significant Decrease in Visual Function
Assessment
Glare
Reduced contrast sensitivity
Impaired near or distance vision
Myopic shift
Myopic Shift | AKA "Second Sight"

Patient History
Hyperopic with recent onset presbyopia.
Clinical Course
Initial improvement in vision followed by decline as cataract progresses.
Myopic shift is most common in
Nuclear Sclerotic Cataract.
Explanation
1. Hyperopic &/or presbyopic patients have trouble focusing at near distances.
- As the patient experiences clinically significant presbyopic changes, their ability to focus at near distance worsens.
2. In the presence of an NSC...
- The nucleus becomes more dense, causing an increase in the refractive index.
3. This "myopic shift" improves the patient's ability to focus at near distances for a limited time.
- Eventually, the NSC progresses and vision worsens.
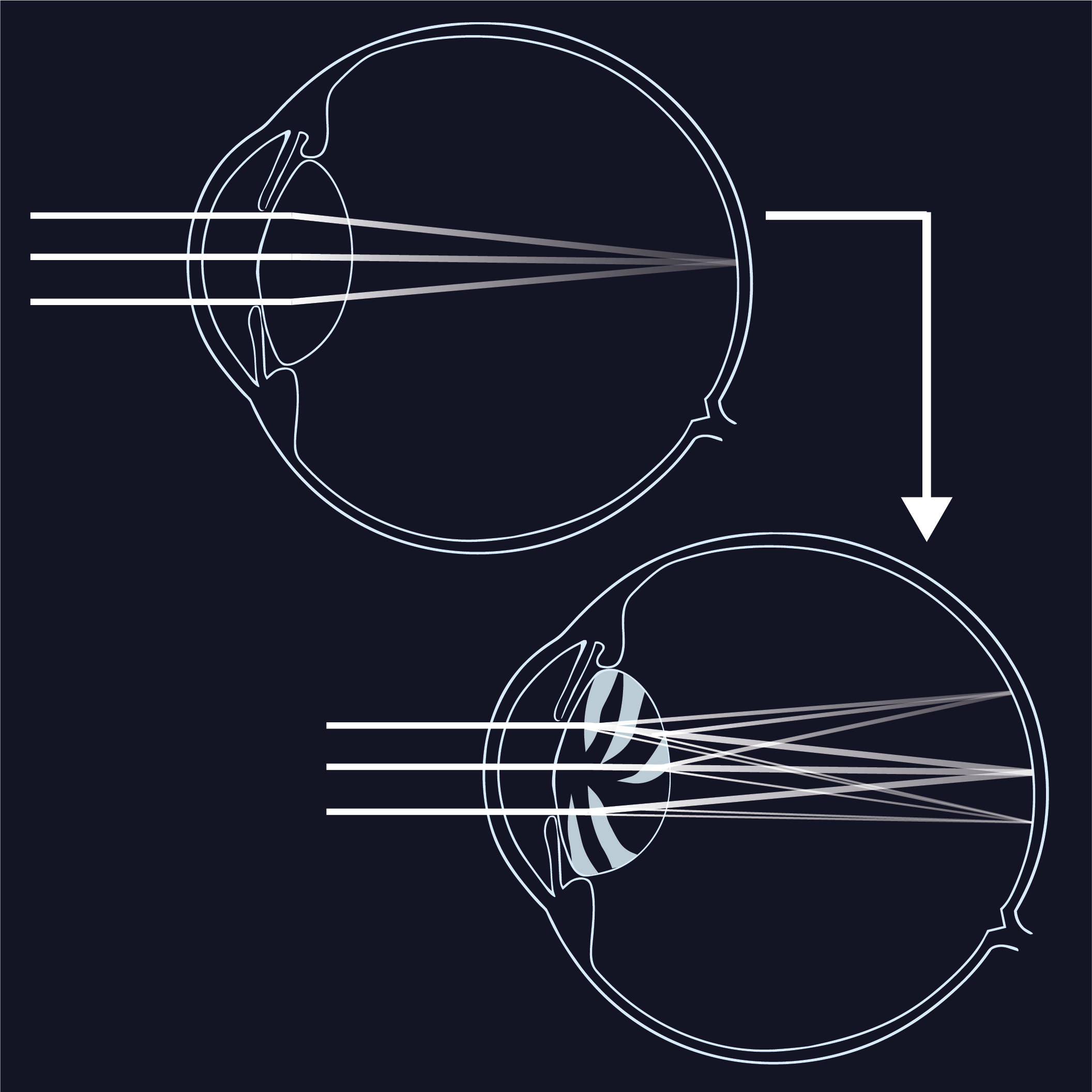
Monocular diplopia or polyopia
Monocular Diplopia or Polyopia
Differential
1. Confirm unilateral etiology.
- Assess cover/uncover, extraocular movements, and visual acuity to rule out neuromuscular etiology.
2. Assess corneal vs lens vs retinal etiology.
- Perform slit lamp exam with attention to corneal surface and cortical lens.
- Corneal topography and tomography should be obtained.
- Consider DFE and OCT of the macula for evidence of an ERM.
Explanation
- Cataracts produce multiple refractile areas at the central lens causing ghost images or true second images to occur.
Monocular diplopia or polyopia is most common in cortical cataracts.
Corneal problems are also a very common cause of monocular diplopia.
Unable to Evaluate Posterior Pathology
Narrow Angles
Lens Dislocation
Clinically Significant Anisometropia
Lens Induced Inflammation or Glaucoma
Etiologies