Lenstar 900 | IOL Master 700 | ARGOS
Measurements
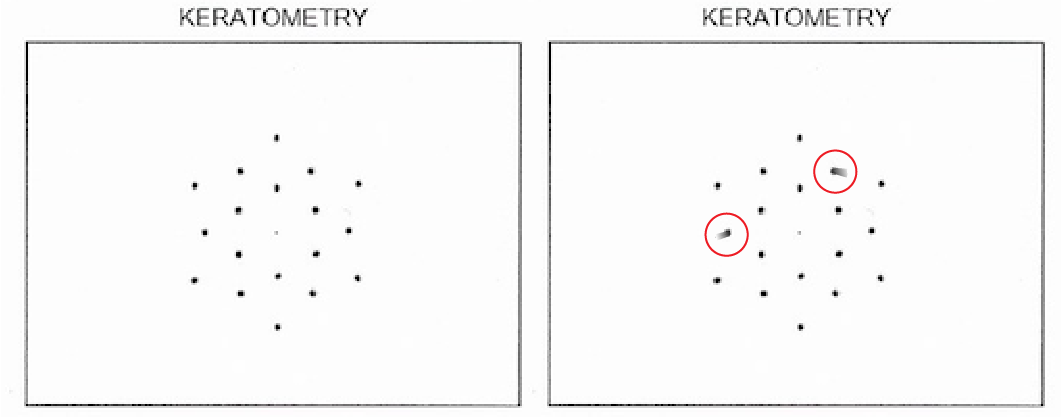
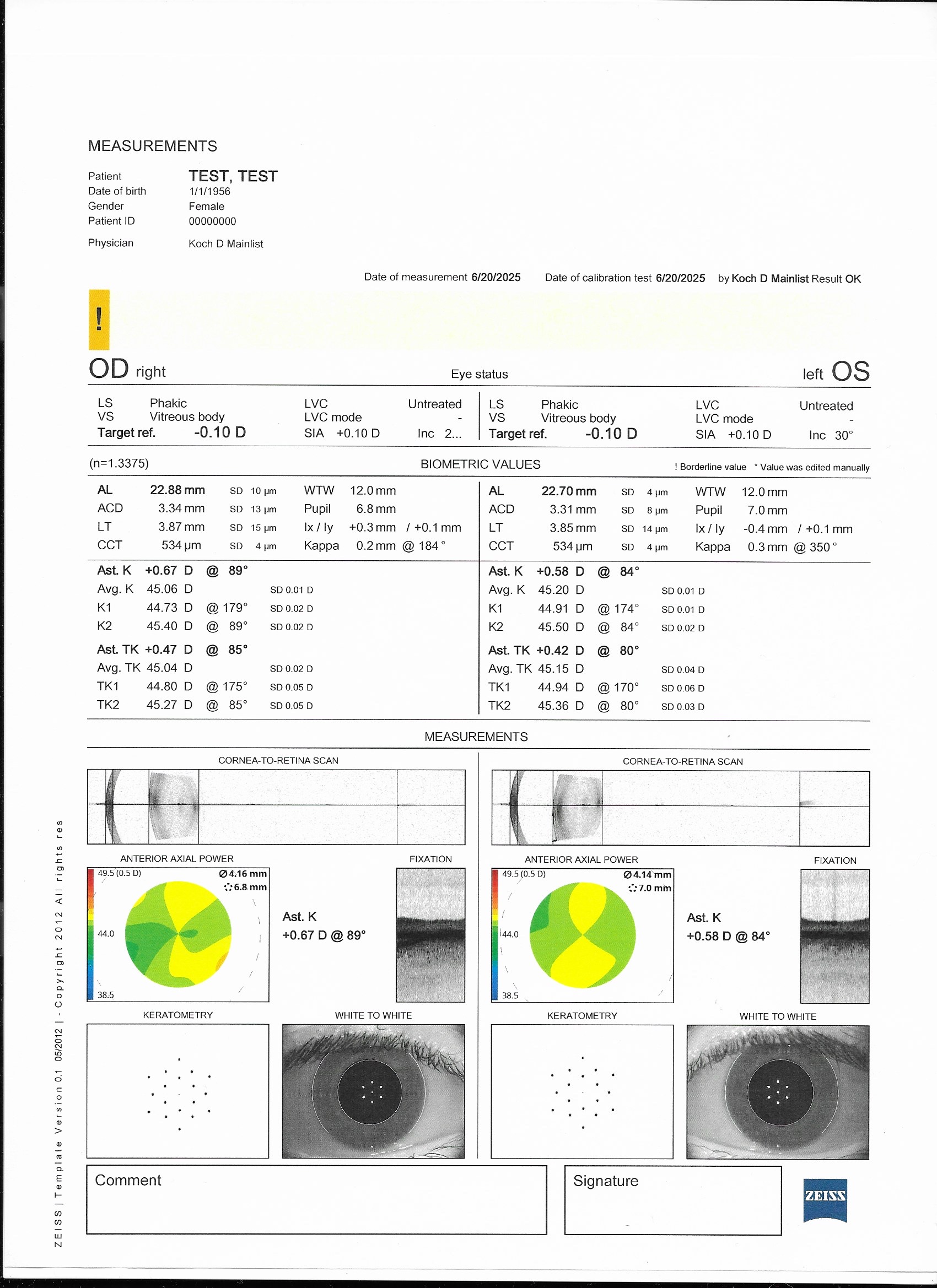
Lens thickness (LT), Central Cornea Thickness (CCT), Axial length (AL), Anterior Chamber Depth (ACD), and Keratometry readings (Ks).
Common Limitations
May have inaccurate or inconsistent measurements in eyes with dry eyes, corneal scarring, PSCs, very mature NSCs, or vitreous hemorrhage.
IOL Master 700
Based on swept source OCT
Better for obtaining measurements in eyes with:
- Dense media (eg, dense cataract)
- Longer axial lengths
Arriola-Villalobos et al 2016
Provides total keratometry (TK) measurements
Direct anterior and posterior corneal curvature.
- Helpful for Toric IOL planning.
**Ensure the IOL formula you put TK into does not already account for posterior corneal astigmatism to avoid overestimating this effect**
Shorter duration to capture scan
Easier for patients with tremors and cognitive impairments to complete.

Lenstar 900
Based on optical low coherence reflectometry
Evaluates 32 points on the cornea.
- Provides more sensitive corneal curvature data.

ARGOS
Based on swept source OCT with segmental refractive index processing
Has an enhanced retinal visualization mode.
- Improves penetration is through dense cataracts.